The stakes are real. The CDC reports that on any given day, approximately 1 in 31 U.S. hospital patients has at least one healthcare-associated infection. Contaminated reusable devices are one documented contributor — and surface finish is one of the variables that determines whether reprocessing actually works.
This article breaks down how surface roughness affects cleanability, which finish types perform best for each device category, and why surface preparation is as critical as the finish itself.
TL;DR
- Ra (surface roughness) is the primary measurable predictor of cleanability — smoother surfaces harbor fewer pathogens and support more reliable cleaning validation
- Biofilms can tolerate disinfectants at concentrations 10 to 1,000 times higher than planktonic bacteria — making rough surfaces a genuine clinical risk
- Electropolishing and passivation are the gold standard for implants and surgical instruments — powder coating suits non-contact equipment
- Surface preparation is non-negotiable — contaminants sealed under a finish create failure points no cleaning protocol can fix
Why Cleanability Is a Critical Surface Finish Requirement
Surface contamination in medical devices is not simply a sterilization problem. A 2023 review of medical-device-associated infections found that contaminated reusable devices can harbor bacterial and fungal species in planktonic, biofilm, and spore forms that survive standard reprocessing. The problem compounds when devices dry between uses — a 2025 Scientific Reports study found that prolonged drying makes soil significantly harder to remove, particularly in occluded geometries like threaded screws, mated surfaces, and lumens.
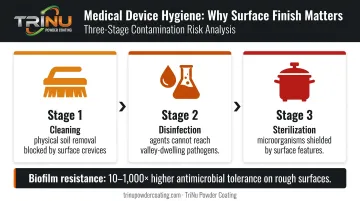
Surface finish affects all three stages of device hygiene:
- Cleaning — physical soil removal is harder on rough surfaces where debris lodges in crevices
- Disinfection — chemical agents cannot reach pathogens protected in surface valleys
- Sterilization — steam and chemical sterilants are less effective when surface features shield microorganisms
Biofilm formation makes this risk compounding. Once bacteria colonize a rough surface and form a biofilm matrix, research shows they can tolerate antimicrobial concentrations 10 to 1,000 times higher than planktonic cells. Rough surfaces give pathogens physical refuge from the interventions designed to eliminate them.
That biological reality is why regulators treat surface finish as a design variable, not a cosmetic one. FDA guidance requires that reprocessing instructions for reusable devices be validated for cleaning, disinfection, and sterilization before reuse — and surface finish is explicitly part of that validation.
How Surface Roughness Directly Affects Cleanability
Ra, Rz, and Why One Number Isn't Enough
Ra (arithmetic average roughness) measures the average height deviation of surface peaks and valleys from a mean line, expressed in micrometers (µm) or microinches (µin). It's the most commonly specified parameter on drawings and inspection reports — but it only tells part of the story.
Two surfaces can have identical Ra values and behave very differently:
- Rz (maximum peak-to-valley height) captures the deepest valleys that matter most for bacterial harboring — a surface with moderate Ra but deep isolated valleys can trap pathogens that a cleaning agent never reaches
- Surface lay (directionality) determines whether cleaning fluid channels across the surface or gets trapped in directional grooves
- Sa (areal surface texture) provides a 3D average height measurement more representative than 2D Ra for complex geometries — ISO 25178-2 defines Sa as the areal counterpart to Ra
For medical device specifications, Ra alone is an incomplete requirement. Drawings that specify Ra without considering Rz or surface lay may pass metrology checks while producing surfaces that fail cleaning validation.
The Roughness-Adhesion Relationship
Peer-reviewed literature on dental implant abutments identifies Ra = 0.2 µm as a meaningful threshold — below that value, further roughness reduction does not significantly reduce plaque accumulation. Yoda et al. cite evidence that bacterial adhesion is primarily driven by surface roughness above Ra = 0.2 µm on biomaterial surfaces.
These findings establish a directional principle: smoother is meaningfully better for bacterial adhesion below a certain threshold. Device-specific Ra requirements should be established through cleaning validation, not assumed from general industry shorthand — and Ra alone still won't tell you whether subsurface geometry creates a separate problem.
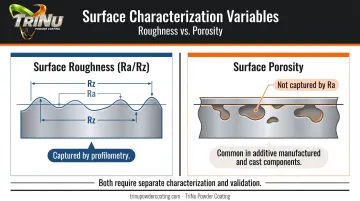
Porosity: A Different Problem Than Roughness
Ra describes surface texture, not internal geometry. Surface porosity — common in additive manufactured (AM) or cast metal components — creates subsurface voids that Ra measurements will not capture. The FDA's additive manufacturing guidance states directly that highly porous regions are expected to be difficult to clean compared with devices made by conventional methods.
Post-processing such as electropolishing or abrasive finishing can close or reduce surface porosity, but until that's done, no cleaning validation result on a porous surface is meaningful. Treat porosity as a distinct process control variable — one that needs its own characterization method and its own validation evidence, separate from roughness assessment.
Metal Surface Finish Types and Their Cleanability Profiles
Electropolishing and Chemical Passivation
Electropolishing removes the outer metal layer electrochemically. The process simultaneously smooths micro-peaks, removes embedded surface contaminants, and creates a chromium-oxide-rich passive layer on stainless steel. The result is a surface that is smoother, more corrosion-resistant, and less reactive than mechanically polished alternatives.
ASTM B912 covers passivation of stainless steels using electropolishing across 200, 300, and 400 series and precipitation-hardened alloys. ASTM F86 governs surface preparation and marking of metallic surgical implants. A 2014 Corrosion Science study confirmed that electropolishing of 316L stainless steel improves corrosion resistance and supports biocompatibility by modifying the surface passive layer.
For AM 316L components, a 2024 study achieved Ra reduction from approximately 12.2 µm to 2.3 µm on upper surfaces using gradient voltage electrochemical polishing — though final Ra targets must be verified on production parts.
Chemical passivation (ASTM A967/AMS2700) removes free iron and surface contaminants through nitric or citric acid treatment. It improves corrosion resistance and surface stability but does not significantly reduce Ra. Passivation is typically a final step after electropolishing or mechanical finishing. It stabilizes the surface chemistry — it does not smooth it.
Mechanical and Abrasive Finishes
Abrasive finishing methods — bead blasting, vibratory finishing, and tumbling — produce uniform matte surfaces that remove burrs and reduce visible contamination. They are appropriate for:
- External instrument surfaces and handles
- Non-contact structural areas
- Components where aesthetics and burr removal matter more than ultra-low Ra
The limitation is embedded media. Glass bead and aluminum oxide particles can become trapped in the surface if post-blast cleaning is inadequate, introducing their own contamination risk. For any surface that will contact patients or fluids, abrasive finishing alone is not a complete solution.
Protective Coatings for Non-Contact Medical Components
Not every medical device surface needs electropolishing. Equipment housings, diagnostic instrument enclosures, support carts, and structural frames have a different requirement profile:
- Chemical resistance to hospital-grade disinfectants
- Impact and abrasion resistance under daily use
- Smooth, nonporous surfaces that support wipe-down cleaning
BIFMA HCF 8.1-2014 cleanability guidance is clear: nonporous, smooth solid surfaces support effective cleaning, while textured surfaces create cleanability problems. The CDC requires that noncritical medical equipment surfaces be disinfected with EPA-registered disinfectants — the finish must be able to withstand repeated exposure to those agents without degrading.
Powder coating, when applied over properly prepared metal, produces a hard, chemically resistant surface that meets these requirements for non-contact components. TriNu Powder Coating provides this service for medical device manufacturers across Tampa Bay, coating device housings, support frames, carts, cabinet enclosures, and OEM sub-assemblies that require durable, cleanable finishes.

The process includes controlled application, verified cure, and documented final inspection before release — meeting the documentation requirements common in regulated manufacturing. Their 10' × 10' × 30' production oven handles large-format components up to 30 feet.
One critical distinction: powder coating and similar protective coatings are appropriate for non-patient-contact components only. Using an equipment housing finish on a fluid-contact or implantable surface is a specification error with regulatory consequences. Finish selection must always start with the device's use classification.
Surface Finish Requirements by Device Category and Standards
| Device Category | Finish Approach | Key Standards |
|---|---|---|
| Implantable devices | Electropolished, lowest achievable Ra, passive layer | ASTM F86, ISO 10993-1, ASTM B912 |
| Reusable surgical instruments | Smooth, burr-free, corrosion-resistant, autoclave-compatible | ASTM F86, ISO 13485 |
| Fluid-contact/cardiovascular devices | Ultra-smooth, validated against thrombosis and protein adhesion risk | ISO 10993-1, device-specific standards |
| AM metal components | Ra + porosity validation required separately | FDA AM guidance |
| External medical equipment | Cleanable, chemically resistant, nonporous coating | CDC/EPA disinfectant compatibility, BIFMA HCF 8.1-2014 |
Two ISO standards govern how manufacturers document and validate surface finish across these categories:
- ISO 13485 requires that manufacturing processes — including surface finishing — be validated within the quality management system. A finish that works in the lab must be demonstrated to consistently achieve the specified condition on actual production parts.
- ISO 10993-1 covers biological evaluation of medical devices and is the framework for assessing biocompatibility, which includes surface chemistry and finish effects on biological response.
Where these standards leave gaps, manufacturers need to fill them explicitly. For passivation specifically, ASTM A967 and AMS2700 govern chemical passivation of stainless steel but do not specify Ra reduction. Roughness matters for most medical device surfaces, which means Ra must be specified and inspected separately from passivation compliance.
Long-term sterilization durability also requires attention at the validation stage. A 2025 Journal of Hospital Infection study tracked AISI 420 stainless steel surfaces through 1,000 cleaning, disinfection, and sterilization cycles. Mechanically brushed surfaces (starting around Ra 0.47 µm) shifted to Ra 0.41 µm after 200 cycles and settled at Ra 0.45 µm after 1,000. Finish degradation is measurable, and design validation must account for it — not just initial qualification.
Surface Preparation: The Foundation of a Cleanable Finish
The cleanability of any surface finish depends entirely on what the surface looked like before that finish was applied. Mill scale, rust, weld spatter, machining oils, and embedded process residues that survive preparation will be sealed into or under the final finish — creating contamination sites that no downstream cleaning protocol can reach.
In production environments, poor preparation drives a disproportionate share of finish failures: delamination, coating breakdown, and contamination pockets that only surface after the component is already in service.
What Controlled Preparation Actually Involves
Abrasive blasting is typically the critical pre-finishing step. Done correctly, it removes surface oxides, scale, and old coatings while creating a controlled anchor profile that improves adhesion of subsequent finishes — whether that's powder coating on equipment housings, passivation on stainless components, or anodizing on aluminum.
The key variables — blast media type, pressure, and angle — all affect the resulting surface profile. Consistency in those parameters is required for repeatable, validated results. Inconsistent prep means inconsistent finish, which means cleaning validation results don't transfer reliably from test parts to production parts.
TriNu Powder Coating's surface preparation process follows this logic directly: material type is assessed first, the appropriate prep method is selected (chemical etching, mechanical etching, or abrasive blasting depending on substrate), and each part is inspected for cleanliness and surface consistency before coating begins.
That structured sequence — not just "blast and coat" — is what makes the downstream finish predictable. For medical equipment manufacturers, a predictable finish means defensible cleaning validation.
Substrate type also matters. Aluminum alloys, stainless steel, and carbon steel each carry different surface characteristics and different preparation requirements:
- Aluminum often requires chemical etching rather than aggressive abrasive blasting to avoid surface damage
- Stainless steel preparation ahead of passivation must not introduce iron contamination from blasting media
- Carbon steel typically tolerates more aggressive mechanical prep, but media selection still affects the final anchor profile

Each of these factors directly determines whether the finished surface performs as specified.
Frequently Asked Questions
What are the different types of surface finishing?
Surface finishing falls into three main categories: mechanical processes (blasting, tumbling, grinding, polishing), chemical and electrochemical processes (electropolishing, passivation, anodizing), and protective coatings (powder coating, parylene, conversion coatings). Selection depends on the component's material, function, and patient-contact classification.
What is a 0.4 Ra surface finish?
Ra 0.4 µm (approximately 16 µin) represents a relatively smooth surface commonly referenced in medical and precision manufacturing specifications. It is frequently cited for surgical instrument and fluid-contact device surfaces as a threshold that limits bacterial adhesion and supports cleaning validation. Confirm the applicable Ra requirement against your device-specific standard and cleaning validation protocol before finalizing specifications.
What is medical device coating?
Medical device coating is any surface treatment applied to improve biocompatibility, corrosion resistance, cleanability, or durability. Common options include electropolishing and passivation for implants and surgical instruments, and powder coating or parylene for external frames and housings — each matched to device classification and patient contact level.
How does surface roughness affect sterilization effectiveness?
Rougher surfaces provide more crevices where bacteria and biofilm can resist sterilization agents. Steam autoclaving, for example, is less effective in pitted or corroded surface areas, and the CDC notes it can also accelerate corrosion in rough surfaces. Lower Ra values reduce these harboring points and support more reliable sterilization across repeated cycles.
Can powder coating be used on medical devices?
Powder coating is appropriate for non-patient-contact components such as equipment frames, housings, support carts, and enclosures — where chemical resistance to hospital disinfectants and durable cleanability are the requirements. It is not appropriate for implantable or fluid-contact device surfaces, which require electropolishing, passivation, or validated biocompatible coatings.
What Ra value is required for implantable medical devices?
No single universal Ra requirement applies to all implantable devices. Peer-reviewed dental implant research identifies Ra = 0.2 µm as a meaningful adhesion threshold, while governing standards such as ASTM F86 and ISO 10993-1 frame the broader evaluation framework. Device-specific requirements should be established through design validation and cleaning validation on production parts.